With >50% Increased Risk to Develop New-Onset Diabetes, Statins are "Starter Drugs" for Post-Menopausal Women. Plus: Younger, Leaner & Asian Women at Greatest Risk
 |
| Image 1: A statin here, some metformin to keep the collateral at bay, add an ACE inhibitor and some anti-coagulant drugs and you have a delicious cocktail of highly profitable pharmaceuticals... |
Keep an eye on your mommy, she might be doing drugs!
As a diligent student of the SuppVersity and thoughtful observer of the blogosphere, I probably won't have to tell you that taking a stating, although they could be life-saving for a infinitesimal percentage of the population, is not as good an idea as the luckily in this part of the world forbidden TV commercials will make. At least for women, the "preventive" use that is so highly advertised by the statin producing pharmaceutical industry, is associated with a 61% increase to develop new-onset diabetes (48% if in addition to age, race and ethnicity, education, cigarette smoking, BMI, physical activity, alcohol intake, energy intake, familiy history of diabetes, and hormone therapy were also considered as confounding factors in the calculation of the hazard ratio), in the 120,173 women without pre-existing cardiovascular disease in the enormous cohort of the Women's Health Initiative study.
 |
| Figure 1: Risk of developing diabetes by statin use among women with and without medical history of cardiovascular disease at baseline; unadjusted, age-and race/ethnicity and multivariate (age, race/ethnicity, education, cigarette smoking, body mass index, physical activity, alcohol intake, energy intake, family history of DM, and hormone therapy use) adjusted hazard ratios (data adapted from Culver. 2011) |
 |
| Figure 2: Association between new-onset diabetes risk and statin use at baseline within different age, race/ethnicity, and BMI subgroups of the 153,840 participants; data shown as unadjusted and multivariate (age, race/ethnicity, education, cigarette smoking, body mass index, physical activity, alcohol intake, energy intake, family history of DM, and hormone therapy use - age, race and BMI were obviously excluded in the respective subgroup analysis) adjusted hazard ratios (data adapted from Culver. 2011) |
If your mama takes statins is a "light-weight" (for her age) and from Asia or the pacific islands, you better get her some Metformin - she probably is going to need it soon...
If you further scrutinize the data in figure 2, it become pretty obvious that the group(s) with the highest risk to develop new-onset diabetes upon being treated with statins are
- women from Asia or the Pacific Islands, with an increased risk of +112% (unadjusted) and +78% (adjusted for the aforementioned variables except from ethnicity, obviously), and
- women with a BMI of <25 kg/m², with an increased risk of +240% (unadjusted) and +89% (adjusted for the aforementioned variables except from BMI, obviously)
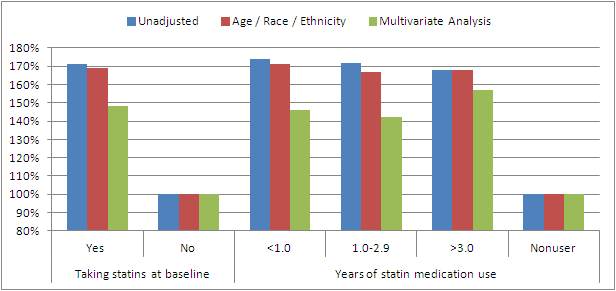 |
| Figure 3: Association between new-onest diabetes risk and statin use at baseline in 153,840 participants; data shown as unadjusted, adjusted for age / race /ethnicity and multivariate (details see figure 1) adjusted hazard ratios (data adapted from Culver. 2011) |
So, let's just hope that the sons and grandsons of these women did not resort to creatine or other dangerous "steroids" from their local GNCs by then! I mean, otherwise it would be likely that they were going on a "roid rage" against their mommy's and granny's doctors, when they see the muscles and brains of their insulin-dependent loved ones wither under the influence of their cholesterol lowering medication.


