Vitamin D3 Supplementation for Older Men & Women Done Right: Dietary Fat Can Increase the Bioavailability by 30%
 |
| Taking vitamin D pills on their own may be less effective than taking them with a meal containing 30% of the calories from fat - at least for older men & women and high doses of vitamin D3 |
Now, half a year later, it appears as if another, previously overlooked variables would force me to reformulate previous recommendations: Age and dosage!
There are many ways to get your vitamin D learn more the SuppVersity

How Much To Take?

Leucine, Insulin & Vitamin D

Vit. D Speeds Up Recovery

Overlooked D-Sources

Vitamin D For Athletes!

Vitamin D Helps Store Fat
- no use of not more than 400 IU vitamin D or 1,000 mg calcium per day,
- serum 25(OH)D level in the range 20 to 29.5 ng/mL (49.9 to 73.6 nmol/L),and
- a body mass index in the range 20 to 29.5 (normal weight)
It's important that the subjects were lean, because (a) the serum vitamin D response may be attenuated by D-storage in the fat tissue and (b) previous studies show that "[o]besity-associated vitamin D insufficiency is likely due to the decreased bioavailability of vitamin D3 from cutaneous and dietary sources because of its deposition in body fat compartments" (Wortsman. 2000).
This was yet not the only difference. Next to the subjects age, the amount of vitamin D3 in the capsules the subjects received differed, as well. While previous studies that reported little to no effect of fat on the absorption of vitamin D3 used small(er) amounts of vitamin D, like 1,000, 2,000 or 5,000 IU per serving, Dawson-Hughes et al. used a single serving of 50,000 IU(!) and thus more than 10x higher dosages than previous studies. |
| Figure 1: Composition of the test breakfast, lunch, and dinner meals, expressed as % of total energy the 50 healthy older adults consumed in the study at hand (Dawson-Hughes. 2014) |
"[The m]eals were provided by the metabolic kitchen and consisted of real food. For example, breakfast consisted of egg whites flavored with small amounts of onion and tomato, fruit, toast, and cranberry juice. The groups were balanced for energy by adjusting the amount of sugar in the cranberry juice (diet or regular juice or a mixture of the two). Protein and fiber were balanced across all groups. MUFA:PUFA was manipulated by adding varying amounts of MUFA (olive oil) and PUFA (corn oil) to achieve a ratio of 1:4 in the low and 4:1 in the high MUFA:PUFA diets. The boxed lunch and the dinner provided to the study subjects on the test day had fat/protein/carbohydrate content similar to that of the test breakfast meals.Importantly, the subjects were required to (a) eat all of the food provided and (b) refrain from pigging out on anything that was not on the menu for the study day.
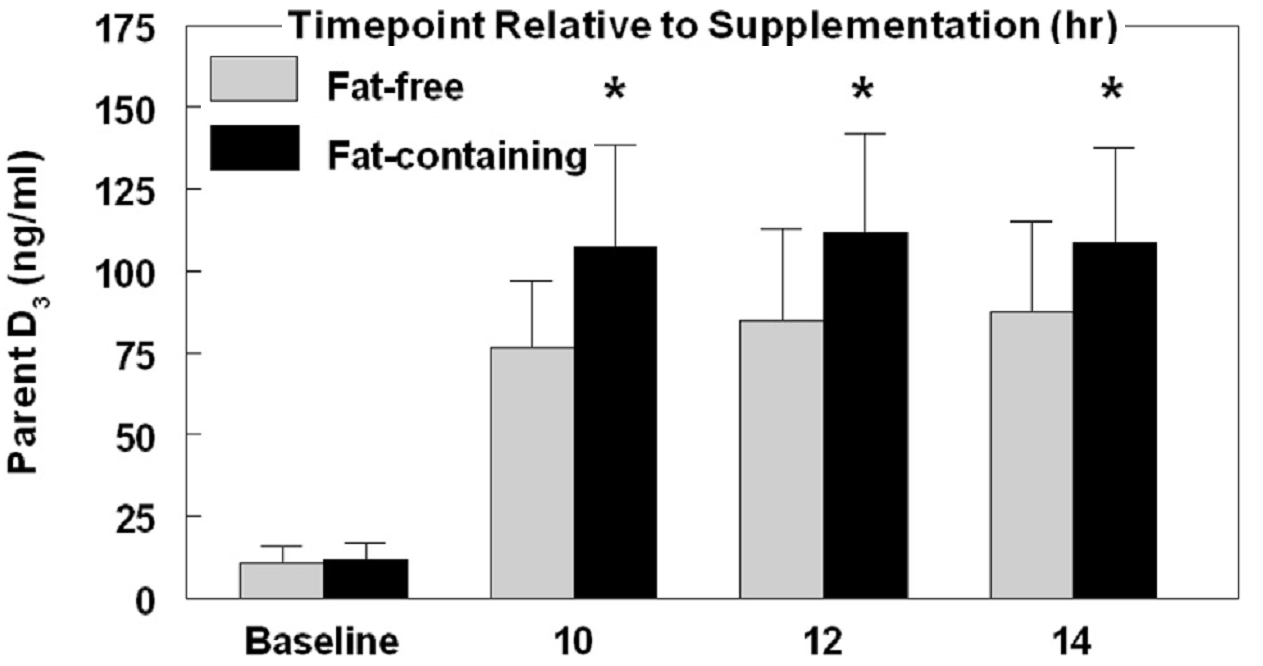 |
| Figure 2: Serum vitamin D3 levels in subjects after consuming fat-free or -containing meals (Dawson-Hughes. 2014) |
- In analyses of
vitamin D absorption at baseline and the three follow-up
time points, there was a significant interaction of fat-free vs
fat-containing meal group with time (P < 0.001). As shown in [figure 2], there was no significant difference in plasma
vitamin D-3 levels at baseline, but the fat-containing meal
group had significantly higher plasma vitamin D-3 concentrations than the fat-free meal group at each time point
thereafter.
At 12 hours, the fat-containing vs fat-free meal mean difference in plasma D-3 concentration was 26.9 ng/mL (95% CI 9.6 to 44.1 ng/mL) (69.9 nmol/L). Differences at the other time points were for 10 hours, 30.5 ng/mL (95% CI 14.4 to 46.7 ng/mL) (79.3 nmol/L) and for 14 hours, 21.3 ng/mL (95% CI 4.6 to 37.9 ng/mL) (55.4 nmol/L).
Keep in mind: Actually, we don't really care about the amount of vitamin D3 in the blood that was measured in the study at hand. What we care about is the impact on the 25-OHD levels and the latter were not tested in the study at hand. Previous studies suggest that using large boluses of vitamin D3 are suboptimal to achieve this goal. Against that background the study design of the study at hand, was not really optimal and didn't access the practically most relevant outcome.
- Vitamin D-3
levels at 12 hours after the dose were 116.0 3 ng/mL
(301.5 nmol/L) in the low MUFA:PUFA group and
104.2 ng/mL (270.8 nmol/L) in the high MUFA:
PUFA group.
Potential covariates, body mass index, total body fat mass, and screening plasma 25(OH)D level were not associated with vitamin D absorption and neither modified the effect of fat on vitamin D absorption.
 |
| Read more about the influence of dietary fat on the bioavailability of vitamin A, D, E & K in "Vitamin A, D, E & K - How Much and What Type of Fat Do You Need to Absorb These Fat Soluble Vitamins?" more |
Furthermore, the previously conducted studies used low not, no-fat meals. Against that background it appears prudent to consume your vitamin D supplements with your meals... and, you are not still eating "no-fat meals", are you?
- Dawson-Hughes, Bess, et al. "Dietary Fat Increases Vitamin D-3 Absorption." Journal of the Academy of Nutrition and Dietetics (2014).
- Niramitmahapanya, Sathit, Susan S. Harris, and Bess Dawson-Hughes. "Type of dietary fat is associated with the 25-hydroxyvitamin D3 increment in response to vitamin D supplementation." The Journal of Clinical Endocrinology & Metabolism 96.10 (2011): 3170-3174.
- Wortsman, Jacobo, et al. "Decreased bioavailability of vitamin D in obesity." The American journal of clinical nutrition 72.3 (2000): 690-693.


