Persistent Fat Loss Involves Diet, Exercise and ... Effective Tryptophan Management!? Here's What You Need to Know
 |
| Cod is one of the foods w/ the highest tryptophan content and a staple in The Rock's get in shape diet - along w/. |
If you have ever tried to lose weight by eating less and exercising more, you will know that this common, but often unsuccessful "obesity solution" can trigger significant mood disturbances (ranging from the literal bad mood to depression) - so significant in fact, that they will make it impossible for you to lose fat.
It may not be exciting, but caffeine can definitely help you lose body fat.

For Caffeine, Timing Matters! 45 Min or More?

Coffee - The Good, Bad & Interesting

Three Cups of Coffee Keep Insulin At Bay

Caffeine's Effect on Testosterone, Estrogen & SHBG

The Coffee³ Ad- vantage: Fat loss, Appetite & Mood

Caffeine Resis- tance - Does It Even Exist?
 |
| Figure 1: Vicious cycle underlying weight gain (yo–yo effect): possible impact of a caloric restriction weight loss diet on mood and hence carbohydrate craving leading to overweight, mediated by modulation of tryptophan metabolism and leptin response (Strasser. 2016) |
 |
| Estimated marginal means (SEs) of mood scores before and after 8, 24, 40, and 52 weeks of energy restriction with a low-carbohydrate, high-fat (LC) diet or a high carbohydrate, low-fat (LF) diet. Beck Depression Inventory score (A), Spielberger State-Trait Anxiety Inventory score (B), and the Profile of Mood States subscales: anger-hostility (C), depression-dejection (D), tension-anxiety (E), fatigue-inertia (F), vigor-activity (G), confusion-bewilderment (H), and total mood disturbance score (I). The asterisk indicates that the score is significantly higher compared with the LF diet (P < .05 | Williams. 2009). |
- moderate physical exercise is a potent stimulus to modulate (reduce/normalize) proinflammatory cytokines, which may in turn beneficially affect TRP levels; for the average obese individual, this form of exercise may thus offer advantages that go way beyond the often overestimated effects on energy expenditure as its effects on TRP coule "be helpful in improving mood status and preventing uncontrolled weight gain" (Strasser. 2016),
- excessive physical exercise as it is unfortunately highly predominant in those seeking to arrive at their "beach body" within a minimal amount of time, however, may actually induce breakdown of TRP when proinflammatory cascades together with TRP-degrading enzyme indoleamine 2,3-dioxygenase-1 are stimulated; needless to say that this may "lead to neuropsychiatric symptoms such as fatigue and low mood" (Strasser. 2016)
sign. and practically relevant changes in your resting metabolic rate (due to "starvation mode"),
No, turkey is not the king of tryptophan, that's COD... or spirulina, which is however not exactly a "food" in my humble opinion (Thrillist). Plus: It accumulates mercury and other elements like a sponge for toxic heavy metals (Johnson. 1986). - low, medium and high intensity exercise (w/ multiple effects), the energy expenditure and effect on intake,
- non-exercise activity thermogenesis (NEAT),
- changes in fat-free mass (e.g. muscle loss or gains) and corresponding changes in energy expenditure, and
- the obvious, energy intake, i.e. the amount (which simply has to be controlled), but also types of food you eat, with some foods having beneficial and other having rather negative effects (learn more in the SuppVersity Overfeeding Review).

"that the small magnitude of weight loss observed from the majority of evaluated exercise interventions is primarily due to low doses of prescribed exercise energy expenditures compounded by a concomitant increase in caloric intake" (Thomas. 2012).There's thus little doubt that dietary restriction(s) and exercise are useful methods to create a negative energy balance - in fact, the existing research clearly indicates that only if you combine both, you will achieve significant and sustainable fat loss.
 |
| Figure 1: The 5HT = serotonin levels in the brain are in control of one's appetite for carbohydrates (Leibowitz. 1998). |
Next to exercise and the previously discussed carbohydrate content, the total amount of energy - or rather the extent of the caloric deficit is probably the most important determinant of the TRP and serotonergic adaptation and its downstream effects:
"In a recent study,18 concentrations of essential amino acid TRP decreased significantly with a caloric restriction weight loss diet, and lowest TRP concentrations were observed in the group of individuals with the lowest calorie intake. The decline of TRP levels can be referred to its reduced intake during caloric restriction diet as it was unrelated to the immune activation status of individuals, which remained unchanged" (Strasser. 2016).Unfortunately, a significant gender differences complicates things: while women experienced the aforementioed lowered the plasma total and free TRP levels that indicate that dieting alters brain serotonin function in women, perhaps as a consequence of reducing the availability of plasma TRP, the effect didn't reach significance in the male subjects of a 1995 study by Walsh,et al. In view of the fact that the study was not a diet only, but a diet + drug challenge study, it is yet difficult to tell how practically relevant said sex-differences are.
How does tryptophan contribute to the yoyo effect? Unfortunately, this is not yet 100% clear. What we know, however, is that a reduced obese (=obese person afters significant weight loss) individual will be hungrier than a similarly lean or overweight peer who has never been obese. Scientists believe that this mismatch of hunger / appetite and the actual energy requirements is due to a messed up configuration of the hypothalamus and hindbrain that serve as the primary control centers for energy balance regulation.
We also know that the same weight loss that sets reduced obese individuals into the "always hungry"-mode, is also associated with significantly increased depressive symptoms (5% weight loss suffice over a four-year period suffice to increase depression, despite benefiting from the expected reductions in cardio-metabolic risk | Jackson. 2014). Needless to say that scientists argue that the detrimental long-term effects (in the short run, the mood usually improves) could be a result of low TRP availability and a lack of serotinin during weight loss.
A state that may limit the production of neurotransmitter serotonin, and thus result in mood disturbances as well as a diminished serotonin functions which will ultimately lead to satiety dysregulation and increased food intake - especially of those foods with the highest reward value, i.e. foods that are high, both in carbohydrates and saturated fats, and which in turn may promote weight gain (Singh. 2014). As Strasser et al. point out in their previously cited 2016, review the loss of tryptophan is only exacerbated by obesity induced increases in the activity of the immunomodulatory enzyme IDO1 during immune activation results which will result in TRP depletion, and will not be restored to normal levels even if the subjects lose significant amounts of weight with bariatric surgery (Brandacher. 2006).
 |
| Complex relationship linking food in-take, mood, and obesity (Singh. 2014). |
A state that may limit the production of neurotransmitter serotonin, and thus result in mood disturbances as well as a diminished serotonin functions which will ultimately lead to satiety dysregulation and increased food intake - especially of those foods with the highest reward value, i.e. foods that are high, both in carbohydrates and saturated fats, and which in turn may promote weight gain (Singh. 2014). As Strasser et al. point out in their previously cited 2016, review the loss of tryptophan is only exacerbated by obesity induced increases in the activity of the immunomodulatory enzyme IDO1 during immune activation results which will result in TRP depletion, and will not be restored to normal levels even if the subjects lose significant amounts of weight with bariatric surgery (Brandacher. 2006).
 |
| Figure 2: Less carbs, less voluntary physical activity - that's a result of Bray's POUNDS LOST Study (Bray. 2012). |
And that's a decrease of ~200kcal (compared to the high carb average protein diet) that may be large and significant enough to make a practical difference over time. Not just because of the 200kcal, obviously but rather because this often moderate physical activity the low-carbers in Bray's study avoided can do what even bariatric surgery failed to do (Brandacher. 2006): counteract the activation of inflammation/IDO1 pathways, which may decrease the susceptibility for mood disturbances and carbohydrate craving by reducing TRP wasting. In fact, animal and human studies have shown that aerobic exercise can stimulate brain serotonin activity and trigger parallel elevations in plasma-free TRP and brain TRP (Strasser: 2016):
- Acute exercise seems to elevate the activity of TRP 5-monooxygenase, the enzyme involved in the rate-limiting step in the synthesis of serotonin, and so leads to an increase in the concentration of serotonin in some areas of the brain, ie, the brain stem and hypothalamus.
- Chronic exercise (30 min/d, six days per week for four weeks) causes neural adaptations by activating not only the synthesis but also the metabolism of serotonin in the cerebral cortex.
- Furthermore, salivary and serum cortisol levels in humans and corticosterone in rats are increased by exercise, and this could induce liver TRP 2,3-dioxygenase, as demonstrated in rats.
 |
| Figure 3: The anti-depressive effects of exercise are at least partly attributable to a rediction in tryptophan metabolism as you can observe them in obese individuals and subsequent increases in KYN and its influx in the brain (Agudelo. 2014). |
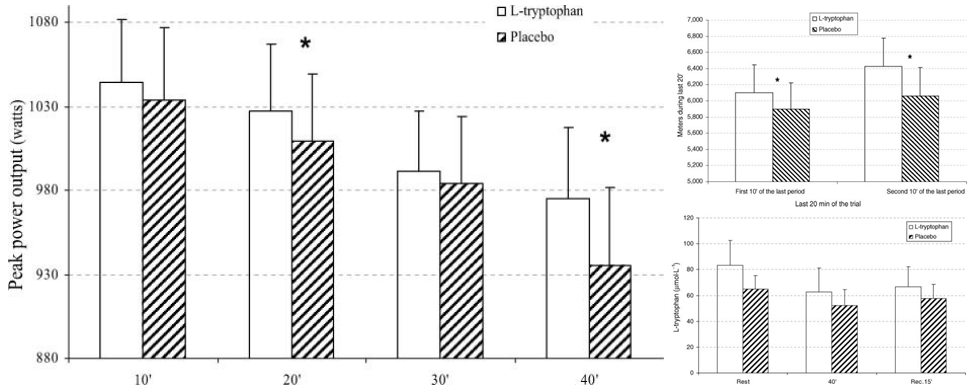 |
| Figure 4: Supplementing with 0.04g/kg body weight tryptophan increases, not decreases, the peak performance and the endurance (as indicated by performance increases at the beginning and end of the last bout) during aerobic work with brief periods of supramaximal intensity that closely mimics the activity typical of team sports (Javierre. 2010). |
"[...] physical exercise could mitigate the biological changes that occur with weight loss (ie, decreased metabolic mass, increased metabolic efficiency, and increased hunger and depression) via both an increase in energy expenditure (with the potential to generate an energy deficit) and the induction of an anti-inflammatory environment (with a subsequent increased release of serotonin)" (Strasser. 2016).In that, future studies will have to show where "good" exercise becomes "too much exercise" and the pro-inflammatory and thus anti-serotonin effects begin to outweigh the previously described anti-inflammatory effects with their beneficial downstream effects on tryptophan metabolism.
So, yes: Even though it would be foolish to ascribe successful weightloss to tryptophan alone, it is hard to ignore the significance of the way this important essential amino acid interacts with diet and exercise in weight or rather fat loss contexts.
During periods of heavy training and or severe dieting, when TRP breakdown is increased and the intake limited, it may thus in fact make sense to provide extra TRP in form of amino acid of high EAA (whey) supplements.
Evidence of benefits comes from studies that show improved mood status and the prevention of uncontrolled weight (re-)gain or neuropsychiatric symptoms (Brzezinsk. 1990) as well as dieting / supplementation studies I discussed in an article from January last year (read it). What may be more important than a sufficient supply of TRP in the diet (and/or supplements, however) is the management of its metabolism.
After all, an increase in TRP breakdown and the accumulation of TRP uptake (into the brain) inhibiting BCAAs in the blood are proven side effects of obesity, of which studies show that they can be controlled by sane amounts of exercise and anything that improves insulin sensitivity, including alpha lipoic acid (Salazar. 2000) and other potent supplemental antioxidants.
Needless to say that this also implies that high(er) carbohydrate intakes can only promote brain serotonin in insulin sensitive, yet not resistant individuals who may eventually be better off on low carb diets until their insulin sensitivity is restored. It would thus be interesting to study if this coincides with the decline in fat loss many people report after 3-6 months on low carbohydrate diets, but I guess that's not the only study that will still have to be done to substantiate the recommendation to (a) get enough dietary TRP, (b) work out regularly, but not like a maniac and (c) don't discard the pro-serotonin effects of carbs if you're insulin sensitive | Comment!
References: |
| Trp and it's metabolite 5-HTP may be particularly useful for female sugar cravings and binges. Since I've discussed these effects in a previous article from 2015, I decided to simply reference it instead of copy + pasting my summary of the existing experi-mental evidence from January 2015. |
Needless to say that this also implies that high(er) carbohydrate intakes can only promote brain serotonin in insulin sensitive, yet not resistant individuals who may eventually be better off on low carb diets until their insulin sensitivity is restored. It would thus be interesting to study if this coincides with the decline in fat loss many people report after 3-6 months on low carbohydrate diets, but I guess that's not the only study that will still have to be done to substantiate the recommendation to (a) get enough dietary TRP, (b) work out regularly, but not like a maniac and (c) don't discard the pro-serotonin effects of carbs if you're insulin sensitive | Comment!
- Brandacher, Gerald, et al. "Bariatric surgery cannot prevent tryptophan depletion due to chronic immune activation in morbidly obese patients." Obesity surgery 16.5 (2006): 541-548.
- Bray, George A., et al. "Effect of diet composition on energy expenditure during weight loss: the POUNDS LOST Study." International journal of obesity 36.3 (2012): 448-455.
- Brzezinski, Amnon, et al. "Plasma concentrations of tryptophan and dieting." BMJ: British Medical Journal 301.6744 (1990): 183.
- Jackson, Sarah E., et al. "Psychological Changes following Weight Loss in Overweight and Obese Adults: A Prospective Cohort Study." PloS one 9.8 (2014): e104552.
- Javierre, C., et al. "L-tryptophan supplementation can decrease fatigue perception during an aerobic exercise with supramaximal intercalated anaerobic bouts in young healthy men." International Journal of Neuroscience 120.5 (2010): 319-327.
- Johnson, Phyllis E., and L. Elliot Shubert. "Accumulation of mercury and other elements by Spirulina (Cyanophyceae)." Nutr Rep Int 34.1063 (1986): 70.
- Leibowitz, Sarah F., and Jesline T. Alexander. "Hypothalamic serotonin in control of eating behavior, meal size, and body weight." Biological psychiatry 44.9 (1998): 851-864.
- Strasser, Barbara, Ken Berger, and Dietmar Fuchs. "Effects of a caloric restriction weight loss diet on tryptophan metabolism and inflammatory biomarkers in overweight adults." European journal of nutrition 54.1 (2015): 101-107.
- Strasser, Barbara, and Dietmar Fuchs. "Diet Versus Exercise in Weight Loss and Maintenance: Focus on Tryptophan." International Journal of Tryptophan Research: IJTR 9 (2016): 9.
- Segura, R., and J. L. Ventura. "Effect of L-tryptophan supplementation on exercise performance." International Journal of Sports Medicine 9.5 (1988): 301-305.
- Thomas, D. M., et al. "Why do individuals not lose more weight from an exercise intervention at a defined dose? An energy balance analysis." Obesity Reviews 13.10 (2012): 835-847.
- Walsh, A. E. S., et al. "Dieting decreases plasma tryptophan and increases the prolactin response to d-fenfluramine in women but not men." Journal of affective disorders 33.2 (1995): 89-97.


