26% Body Fat, Zero Lean Mass Loss W/ HIIT + 3x500mg Green Tea Supp in 10Wks | Is EGCG Liver-Toxic?
 |
| Lean, not skinny: In the long run HIIT + GTE could take you there, but there's one caveat... at least w/ the green tea. |
An attractive alternative would be (i) not having to diet, (ii) not having to do endless cardio sessions and (iii) having a fat loss supplement that actually works.
Looking for more cutting edge exercise and supplementation science?

Vitargo, Red Bull, Creatine & More | ISSN'15 #1

Pump Supps & Synephrine & X | ISSN'15 #2

High Protein, Body Comp & X | ISSN'15 #3

Keto Diet Re- search Update | ISSN'15 #4

The Misquantified Self & More | ISSN'15 #5

BCAA, Cholos-true, Probiotics & Co | ISSN'15 #6
Well, guess what, Afzalpour et al. have an ahead-of-print paper they tagged with the keywords "HIIT;Vitargo, Red Bull, Creatine & More | ISSN'15 #1
Pump Supps & Synephrine & X | ISSN'15 #2
High Protein, Body Comp & X | ISSN'15 #3
Keto Diet Re- search Update | ISSN'15 #4
The Misquantified Self & More | ISSN'15 #5
BCAA, Cholos-true, Probiotics & Co | ISSN'15 #6
Catechins; SRIT1; PGC-1 "(Afzalpour. 2017) that appears to suggest that this 'attractive alternative' does actually exist - at least for those women who have the most body fat to complain about for whom the scientists speculated that it could be the combination of "green tea consumption along with HIIT training" that "would improve body composition in overweight individuals and would show significantly greater improvements compared green tea consumption or HIIT training alone" (Afzalpour. 2017) - without dieting (or I should say: without prescribed dieting, the scientists did not access the women's food intake over the 10-week period; there was just a baseline reading)!
 |
| Table: Anthropometric characteristics of the subjects in the three groups (Afzalpou. 2017); note: there were no significant baseline differences in body composition and fitness between the three groups of young women. |
- HIIT plus 1.5g/day green tea in 3x500mg servings with meals (HIIT+G),
- HIIT plus placebo (HIIT), and
- no training and supplementation control group (CON).
"[t]he protocol of HIIT required the participants to finish a determined path (20 meters) with their maximum speed within 30 seconds. The starting point of the test was exactly in the middle of the obstacles, i.e., 10 meters from each obstacle.
Figure 1: Overview of the HIIT parcours and the periodization scheme (Afzalpour. 2017).

The training included running from the middle line to the first obstacle and then returning a 20-meter path to the second obstacle. After each run, there was an active rest for 30 seconds (Figure 1).
In the first and second weeks, the training was performed with 4 repeats, in the third and fourth weeks with 5 repeats, in the fifth and sixth weeks with 6 repeats, in the seventh and eight weeks with 7 repeats, and in the ninth and tenth weeks with 8 repeats (Figure 1). In each session before the training protocol, the participants had [to] warm up for 5—10 minutes, and they cooled down for 5—10 minutes at the end of each session." (Afzalpour. 2017).The intensity of training within the activity was controlled by measuring the heart rate during
the activity by pulse meter and using maximum heart rate formula (220-age). Besides, the Borg scale (6—20) was used to ensure greater control over the intensity of training.
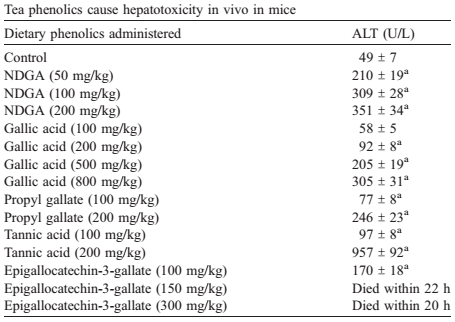 |
| Rodent studies clearly confirm the hepatoxicity of high doses of green tea; with the often-hailed EGCG having the most significant impact on the liver health of mice - with death being a consequence of the injection of a human-equivalent-dose of "only" 12mg/kg, or 850mg - luckily, the oral bioavailability of EGCG is low (Galati. 2006). |
More recently, however, there have 24 case-reports of liver problems in response to the consumption of green tea supplements in man from 1999 to 2009, only (Mazzanti. 2009) - a response of which scientists say that it is due to (-)-epigallocatechin gallate (EGCG) or its metabolites "which, under particular conditions related to the patient’s metabolism, can induce oxidative stress in the liver" (Mazzanti. 2009).
Whether that's actually the case in the human case studies is particularly difficult to tell (Molinari. 2006), because it is well possible that "[i]n a few cases, toxicity related to concomitant medications could also be involved" (Mazzanti. 2009) - especially because EGCG messes significantly with the cytochrome P450 cascade, inhibiting, CYP1A2, CYP2D6, CYP2C9, and CYP3A4, which metabolizes not just all sorts of anti-depressive drugs, but also estrogen and could potentially explain the T-reductions in the previously mentioned 2011 study. In addition to that, a more recent series of studies (James. 2016) suggests that
"EGCG treatment induced hepatotoxicity [is dose dependent] and it induced oxidative stress by inhibiting antioxidant response. Mitochondrial function was impaired based on reduced biogenesis and inhibition of complexes following EGCG treatment." (James. 2016)As bad as it may sound, this can (a) explain why it worked in the study at hand - practically speaking it did the opposite of what the anti-oxidants which hampered the gains in Bjornson et al. (2015 | discussed in detail, here), did it added to the pressure to adapt - and (b) and must be reconciled with the already low and chronically decreasing bioavailability of EGCG with chronic administration.
One important advice I want to give you at this point is still: do not fall for the notion that 'more helps more' (toxicity of really high doses of GTE in rodents has been proven multiple times), do not buy a pure EGCG product and stop using your green tea supplements if you notice the first symptoms of liver problems (usually otherwise inexplicable fatigue).
 |
| Figure 2: Total changes (kg) in body fat and total lean mass and corresponding relative changes (in %) above the bars. |
 |
| Figure 3: Relative changes in SIRT1, PGC-1A activity and physical fitness as measured by the women's VO2-max. |
 |
| Don't get me wrong: There are a lot of studies showing beneficial effects of green tea extracts, including the recently discussed study showing that "Green Tea Extract Reduces the Amount of Insulin You Need to Store Your PWO Carbs by ~20%". Unfor-tunately, its probably individual liver-damaging effects are being observed in more and more studies, too. |
Now, the question remains: Is it worth taking the (probably small, but existing) risk of putting your liver health in jeopardy? You got to answer this question for yourself, but if you're having liver problems already, high dose EGCG supplements should IMHO be a no-go... the good news is: since the authors didn't report any EGCG standardization for their supplement, it is very likely that they are also not necessary and drinking green tea, which is a way of preparing your own hot water extract from tea, alone, with every meal could boost your fat loss and is associated w/ a reduced risk of liver cancer (Ni. 2017) | Comment!
- Afzalpour, M. E., E. Ghasemi, and A. Zarban. "Effects of 10 weeks of high intensity interval training and green tea supplementation on serum levels of Sirtuin-1 and peroxisome proliferator-activated receptor gamma co-activator 1-alpha in overweight women." Science & Sports (2017).
- Galati, Giuseppe, et al. "Cellular and in vivo hepatotoxicity caused by green tea phenolic acids and catechins." Free Radical Biology and Medicine 40.4 (2006): 570-580.
- James, Karma. Effect of dietary pretreatment and obesity on (-)-epigallocatechin-3-gallate (EGCG) mediated hepatotoxicity and the underlying mechanism. Diss. The Pennsylvania State University, 2016.
- Mazzanti, Gabriela, et al. "Hepatotoxicity from green tea: a review of the literature and two unpublished cases." European journal of clinical pharmacology 65.4 (2009): 331-341.
- Molinari, Michele, et al. "Acute liver failure induced by green tea extracts: case report and review of the literature." Liver transplantation 12.12 (2006): 1892-1895.
- Ni, Chen-Xu, et al. "Green Tea Consumption and the Risk of Liver Cancer: A Meta-Analysis." Nutrition and Cancer (2017): 1-10.


