'Survival of the Fittest!' Large-Scale Study Backs Classic Evolutionary Paradigm - Being Unfit Worse Than Smoking | Plus: Fit/Unfit - What are You + What Can You do About it?
 |
| Even the difference between having 'below ' vs. 'above average' fitness levels amounts to the same 1.4-fold increase in mortality risk the scientists calculated for smoking cigarettes. |
However, upon closer scrutiny, it turned out that both, the hazard ratio for smoking vs. non-smoking, which is 1.41 (p < 0.001), and the hazard ratio for elite vs. low fitness, which is 5.05 (p < 0.01) and hence 3.6 times higher, were based on analyses of the same dataset - cool!
Bicarbonate can help you train at intensities that promote VO2Max gains even on an 'elite' level:

Caffeine + Bicarb Make Champions

Bicarb + Asp = Muscle Magic!?

NaCHO3 & Leg Days're a Breeze

+100% Anaerobic Endurance

Bicarb Buffers Creatine

Instant 14% HIIT Boost
 |
| Figure 1: Risk-Adjusted All-Cause Mortality | Adjusted hazard ratios (HRs) for all-cause mortality compared with low performers in all patients (A) and by sex (B) (P values are for comparisons with low performers | Mandsager 2018). |
Moreover, Mandsager found that even small differences in fitness, as well as differences among the fittest 20%, went hand in hand with a practically relevant reduction in mortality risk.
Over the course of the ~8-year period Mandsager et al. monitored their subjects, the researchers did, for example, observe the same 1.4-fold increase in mortality risk for people with 'below' and 'above average' fitness levels as they did for smokers vs. non-smokers.
 |
| Table 1: Group classifications by cardiorespiratory fitness used in the study by Mandsager et al. 2018; marked in green is a 30-year-old male with a 'high' fitness level. |
The latter had been determined for all 122 007 patients in different exercise tests (the specific tests were chosen according to the patients' individual health status). Table 1 gives you an overview of the VO2 values in METs (1 MET = 3.5 mlO2/kgbodyWeight/min, hence 13.7 METS = 47.95 mlO2/kgbodyWeight/min) and the corresponding fitness level.
You want tangible examples? Well, a 30-year-old who will be exhausted after walking (1.7 mph) on a treadmill with an incline that progressed from 0-10% in 3-minute intervals for 9 minutes would fall into the 'low' fitness category. The same 30-year-old would be categorized as 'highly' fit if he managed to stay on the treadmill for 18 minutes, progressing, again in 3-minute intervals, from walking (1.7mph) at 0% incline to running at 4.2 mph at an incline of 16% before he'd be totally exhausted (see infobox "How do you estimate your fitness" for more info).
 |
| Figure 2: Plot of the hazard ratios for being in the 'low' (left) and 'high' (right) fitness versus all other categories (based on Mandsager 2018); note: everything above the red demarcation line at HR = 1.0 indicates that being in the corresponding fitness category vs. 'low' (left) and 'high' (right) is protective, everything below the red line indicates that being in this category is associated w/ a greater mortality hazard compared to having a 'low' or 'high' fitness level, respectively. |
Now, your most important question probably is: Where do I stand 'fitness-wise'?
Well, to answer this question you'd have to do a treadmill maximal exercise test like the one(s) the subjects in the study at hand did. Since, different tests were used - according to what the participants' fitness/health would allow - your best bet here is the so-called "Bruce test".
 |
| Table 2: Overview of the speed and grade at which you have to run on the treadmill during the Bruce test (University of British Columbia) - the stages are completed subsequently. Your outcome is calculated based on the cumulative time you spent on the treadmill as VO2 max = 14.8 - (1.379 x T) + (0.451 x T²) - (0.012 x T³). With that being said, you can also use a tool like QxMD to calculate your fitness level. |
Like every other maximal exercise test, the Bruce test requires you to run on a treadmill (tests with cycle ergometers and other 'cardio' equipment are also possible) while the speed and incline of the treadmill, you're running on, is increased in 3-minute intervals (see Table 2). The test ends when you cannot keep up with the pace, any longer. Your age, sex, and the stage you've made it to will then allow you to estimate your VO2Max.
Let's consider an example: Say you are 30 years-old male, did an incremental running test and were exhausted after 16 minutes, when you were running at a speed of 4.2mph at an incline of 16%... a calculator like the one from OxMD would then tell you that your capacity is ~14.64 mL/kg/min METs, which is significantly better than the predicted average for a 30-year old 11.4 mL/kg/min METs.
| To actually measure your VO2Max, which was the measure of fitness that was used in the study at hand, you would need a treadmill and a metabolic cart as it is shown in the video, but you can estimate it using just the treadmill. |
There's still room for improvement, though; if you achieved the 'elite' level (VO2Max of >15ml/kg/min METs) you'd have an even lower mortality hazard than those in the 'high fitness' category - a non-significant (p = 0.09) improvement of -19%, as the corresponding sex-specific data from the FT (sex-specific values are not plotted in Figure 3) suggests. By the way, with the same fitness values your likewise imaginary 25-year-old girlfriend would not just already be at the 'elite' level, she would also record a borderline significant -35% (p = 0.06) reduction in all-cause mortality compared to an already fit (female) friend in the 'high' fitness category.
I guess, by now you'll begin to realize that both one's fitness, as well as the reduction in mortality risk one can expect based on the results of the study heavily, depend on various confounding factors, i.e. one's sex, age, comorbidities, etc.
DO not confuse the time you spend exercising with the fitness level you have! If you read the headlines, you will find that several websites chose similar titles like "No Such Thing as Too Much Exercise, Study Finds" - a headline that (falsely) suggests that it's the amount of and hence the time you spend exercising that's at the heart of the reduced mortality hazard in the study under review.
(Un?)fortunately, the time you spend on the treadmill, in the gym or running, walking, and cycling outdoors is at best a proxy, but by no means a valid predictor of your physical fitness. I would bet my favorite pair of gym-shoes (and yes, I love squatting in them) that there's more than one SuppVersity reader who would achieve higher fitness levels - in this context estimated VO2max values - if he/she trained less not more. It would thus be haphazard to increase your training volume beyond your adaptational capacity to reduce your mortality risk - the opposite could happen!
Yes, studies in (former) elite athletes do indeed confirm an increased life expectancy (1-8 years, depending on the study, see Table 3 | Reimers 2012). However, unlike the weekend warriors at your local gym, these athletes have trainers who make sure that they don't out-train their own recovery ability and continuously improve their VO2max (fitness-)levels.
Scientists are well aware of this potentially life-threatening disconnect between actual physical activity and the estimated VO2Max values (~physical fitness). John Higgins, MD, MBA, MPhil, from the Lyndon B. Johnson General Hospital in Houston, for example, warns that the study he was not actively involved cannot account for possible adverse effects of (too) intense training and highlights: "[W]e cannot exclude [...] issues with overtraining or overdoing the exercise to extremes with respect to total weekly volume, and not allowing an appropriate recovery after exercise"(MedPageToday) - if it applies at all, the overtly simplistic mantra "more helps more" does therefore only apply to physical fitness, yet not to the amount of effort you invest in achieving it.
The latter is an important insight, as it can also explain why some of the effects the scientists observed when they compared the 'high' vs. 'elite' fitness group did not reach statistical significance. We've seen that earlier in our example. If you thought that was bizarre, what do you make of the fact that exactly those of whom you'd usually suspect that they'd benefit most, i.e. people with comorbidities such as CAD [=Coronary artery disease], diabetes, hypertension, or hyperlipidemia (i.e. high blood lipids) do not seem to benefit from 'elite' fitness (see Figure 3).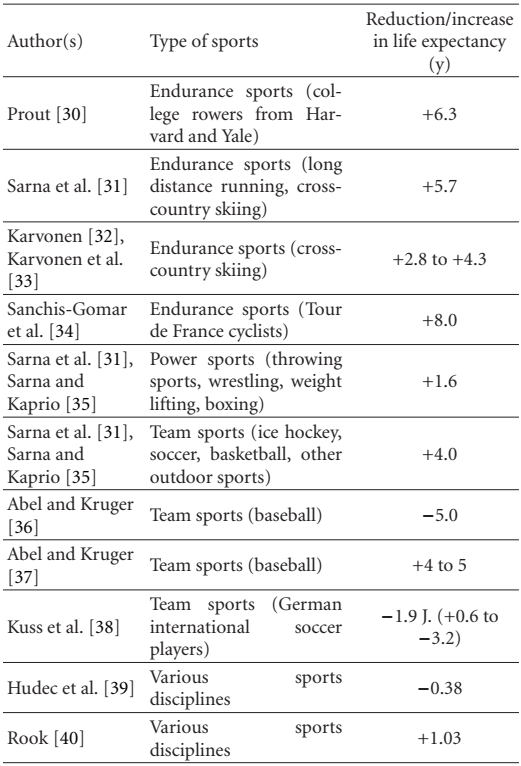 |
| Table 3: Case-control studies presenting life expectancy of (former) athletes compared to that of control subjects (Reimers 2012). |
Yes, studies in (former) elite athletes do indeed confirm an increased life expectancy (1-8 years, depending on the study, see Table 3 | Reimers 2012). However, unlike the weekend warriors at your local gym, these athletes have trainers who make sure that they don't out-train their own recovery ability and continuously improve their VO2max (fitness-)levels.
Scientists are well aware of this potentially life-threatening disconnect between actual physical activity and the estimated VO2Max values (~physical fitness). John Higgins, MD, MBA, MPhil, from the Lyndon B. Johnson General Hospital in Houston, for example, warns that the study he was not actively involved cannot account for possible adverse effects of (too) intense training and highlights: "[W]e cannot exclude [...] issues with overtraining or overdoing the exercise to extremes with respect to total weekly volume, and not allowing an appropriate recovery after exercise"(MedPageToday) - if it applies at all, the overtly simplistic mantra "more helps more" does therefore only apply to physical fitness, yet not to the amount of effort you invest in achieving it.
 |
| Figure 3: Risk reduction in subjects with elite vs. high fitness status; only full bars represent sign. effects (Mandsager 2018) |
 |
| What's the Optimal HIIT Protocol for Trained Individuals? 48 x 10s or 8 x 60s for Fitness + Improved Body Composition? Find out! |
Now this does mean that #HIIT (vs. #cardio) is the more time-efficient exercise modality to increase your fitness (Helgerud 2007), it is yet - and people tend to forget that these days - not the only way of upgrading your fitness from 'above average', where I hope most of you will be now, to 'high'. Both, the tried and proven "steady-state" training (albeit at challenging intensities of 70%-85% for long durations), as well as an intense, fast-paced resistance training, have the potential of increasing one's VOMax significantly (note: for the latter VO2max increases will probably only occur in rather untrained individuals | see Ozaki 2013).
Irrespective of the mode of exercise you use, there's one thing you should keep in mind: The fitness of the subjects in the study at hand was tested only at baseline, it is thus not clear how long you'd have to stay at a given (improved) fitness level to reap the corresponding mortality benefits.
 |
| Figure 3: Number of subjects classified as having a "low", "below average", "average", "high", and "elite" fitness levels; see Table 1 for what the fitness levels mean in METs (plotted based on Mandsager 2018). |
"[t]he prevalence of associated comorbidities decreased significantly with increasing performance [and what's interesting] with the exception of hyperlipidemia, which was present in 31.6% (1128 of 3570) of elite performers and only 25.1% (7323 of 29 181) of low performers (P < .001)" (Mandsager 2018).If you take another look at the striped bars, which represent non-significant differences, in Figure 3, you will find that these bars refer to the same groups, the scientists mentioned in the quote: subjects with CAD, diabetes, high blood lipids, and normal blood pressure values, i.e. those people who were under-represented in the elite fitness group. Accordingly, the lack of statistical significance doesn't really come as a surprise... and if that's not motivating enough: the 'elite' vs. 'high' fitness advantage for the whole group was 22% and statistically significant (p = 0.02).
 |
| If you are too lazy to upgrade and maintain your fitness level, you may be interested in my article and interview about "The Vampire Approach to Longevity" from April 2018, an article + SHR interview in which I discuss the use of literally 'young blood' injections for life-extension purposes | read more |
You can probably answer this allegedly populist question on your own and would thus like to point out that the mere size of the study is not a sufficient predictor of the validity, relevance, and explanatory power.
In this regard, the authors highlight the following: "The degree to which high CRF [cardiorespiratory fitness] preselects patients with lower mortality vs causes a reduction in mortality is not discernible from our study" (Mandsager 2018).
Or, as I would phrase it: Since we're dealing with a retrospective observational study, we are not allowed to infer a causal relationship between the subjects' fitness levels and their mortality risk. What we can do, however, is to call the existence of a causal link a "reasonable assumption" - an assumption of which we know that it is unlikely to be either challenged or confirmed in an 8-10-year longitudinal, large-scale, randomized clinical trial in subjects that were not chosen, because they were advised to participate in an exercise test at the Cleveland Clinic. Why's that? Well such a trial would cost millions of research dollars and face a good dozen of severe obstacles ranging from ethical issues to very practical questions such as: "How do I ensure minimal dropouts and the maintenance of the initial fitness level?" | Comment!
- Gormley, Shannan E., et al. "Effect of intensity of aerobic training on V˙ O2max." Medicine & Science in Sports & Exercise 40.7 (2008): 1336-1343.
- Helgerud, Jan, et al. "Aerobic high-intensity intervals improve V˙ O2max more than moderate training." Medicine & Science in Sports & Exercise 39.4 (2007): 665-671.
- Mandsager K, Harb S, Cremer P, Phelan D, Nissen SE, Jaber W. "Association of Cardiorespiratory Fitness With Long-term Mortality Among Adults Undergoing Exercise Treadmill Testing." JAMA Network Open. 1.6 (2018):e183605. doi:10.1001/jamanetworkopen.2018.3605
- Ozaki, Hayao, et al. "Resistance training induced increase in VO 2 max in young and older subjects." European Review of Aging and Physical Activity 10.2 (2013): 107.
- Reimers, Carl D., G. Knapp, and Anne Kerstin Reimers. "Does physical activity increase life expectancy? A review of the literature." Journal of aging research 2012 (2012).
- Scribbans, Trisha D., et al. "The effect of training intensity on VO2max in young healthy adults: A meta-regression and meta-analysis." International journal of exercise science 9.2 (2016): 230.


