There is More To Glucose Control Than Carbohydrates (2/?): Non-Carbohydrate Nutrients And Their Effects On Blood Glucose Management ➲ SFA, MUFA PUFA, TFA & Co - Fats!
 |
| Some say "fat is a mistake" others say "it was our fattest mistake to believe just that" - who is right? Or are things eventually more complicated than that? |
This week we will make a fat transition (all puns intended) to the 2nd macronutrient that exerts non-carbohydrate dependent effects on glucose homeostasis: FAT!
We have known for decades that the acute glycemic response is affected by the fat content of the diet.
As my German "friends", Martina Heer and Sarah Egert, whose recent paper in the scientific journal Diabetes/Metabolism Research and Reviews inspired me to write this article series point out, a recent meta-analysis of the existing literature on low-carbohydrate + high-fat diets suggests that these diets, unlike high-carbohydrate and high glycemic index diets, may be effective in improving glycemic control, weight, and lipid profiles (Schwingshackl. 2011).
You can learn more about this topic at the SuppVersity

Proteins, Peptides & Blood Glucose

SFA, MUFA, PUFA & Blood Glucose

Read these ➲ while waiting


16 Weeks High Fat Diet

Fat to Blunt Insulin?
We all know that there is hardly a better way to reduce blood glucose levels than not eating carbohydrates, but if you look at the title of this series and my goal to present an analysis of the effects of non-carbohydrate nutrients on blood glucose homeastasis in humans, it should be obvious that low carb diets must be excluded from this overview. What we will focus on in this installment is thus
- the general effect of dietary fat on the absorption, appearance and clearance of glucose from the bloodstream, and
- the different effects of saturated, monounsaturated, and polyunsaturated short- and long-chain fatty acids on glucose homeostasis
Where are the short chains? If you are honest, this is an unwarranted question. We are, after all talking about "non-carbohydrate nurtients" from your diet, here and last time I checked, the production of short chain fatty acids in our guts required dietary carbohydrates. If we discard the 3-4% of butyrate quality butter, you will thus have to consume resistant starches to benefit from the proven anti-diabetic, anti-obesity effects that is brought about by the interaction of gut derived short chain fatty acids with "their" receptor, ie. GPR43 (den Besten. 2013; Kimura. 2013).
The ratio of these monounsaturated, polyunsaturated and saturated fatty acids in our diet determines our own molecular built, meaning: The dietary acid composition of our diet has both acute mechanistic, and chronic structural effects on our cells, which are mediated by the storage of fatty acids in tissues and cell
membranes (Carlson. 1986).
A high intake of trans-fats for example will lead to an accumulation of trans-isomers of linoleic acid in the heart and a highly significant 50% risk increase for cardiac arrest (Lemaitre. 2002).
27nmol/L LDL Per 1% Reduction in Trans Fat Intake | learn more - A high concentration of linoleic acid (n-6) in the erythrocyte membrane has been shown to be negatively, a high palmitic acid content positively associated with incident type 2 diabetes in 1346 Finnish men aged 45–73y researchers from the University of Eastern Finland followed for 5-years in recently conducted a population-based study (note: The researchers detected no protective effect of omega-3 fats; cf. Mahendran. 2014).
In the six years that have passed since the overview by Risérus et al. (2008) Heer and Egert cite in their paper has been published, we have learned much about these direct effects. You all know the effects fish oil, conjugated linoleic acid and co have on the peroxisome proliferator-activated receptors (PPARs) and the corresponding downstream effects on glucose uptake and the storage of superfluous energy in the adipose organ (Kota. 2005. Grygiel-Górniak. 2014)."More recent experimental data also point toward other mechanisms which involve direct regulatory effects on gene expression and enzyme activity.
Fatty acid ⇆ PPAR interaction (Kota. 2005)
For example, in vitro studies and studies in animal models suggest that fatty acids could act directly on insulin-sensitive tissues (Risérus. 2008)." (Heer. 2014)

PUFAs, PPARs and the key to becoming a healthy obese individual
According to the most recent review of the literature, the PPAR-gamma receptor which is activated primarily by unsaturated fatty acid and their metabolites (15- hydroxy eicosatetraenoic acid, 9- and 13- hydroxy octadecadienoic acid, 15-deoxy 12,14-prostaglandin J2, and prostaglandin PGJ2), is the master regulator of glucose homeostasis and lipid storage. Against that background it is no wonder that Risérus concludes his previously cited review on the note:
"Substituting saturated fat with unsaturated fat seems to have beneficial effects on insulin sensitivity, although the clinical significance of modifying fat quality alone is still unclear." (Risérus. 2008)It's after all an increase in insulin sensitivity that is - at least in the chronic overfeeding scenario, we call the "standard American diet" - an increase in insulin sensitivity that is paid for with increased adiposity - a phenomenon that's related to the pro-adipogenic effects of PPAR-gamma and one that diminishes the usefulness of thiazolidinediones like pioglitazone, which are mostly pan(=all) agonists of the peroxisome proliferator-activated receptors, in the battle against diabetes. At least, if you share my opinion and think that treating an already overweight diabetic with a drug that will lead to significant weight gain (Khan. 2002) could do more harm than good in the long run.
The fact that the anti-diabetes effects of PUFAs are mediated by their adipogenic effects does not mean that you have the choice between pest and cholera, but the PUFA induced increase in insulin will always be a double-edged sword, as long as you are consuming significantly more energy than you're expending.
Still, if our main concern is blood glucose management in an overfeeding scenario (=the Western real word), the international recommendations to reduce the intake of saturated fatty acids (SFA) to ≤10% of total energy intake (Aranceta. 2012) do appear warranted. And if replacing them with carbohydrates is not an option, because (a) we are talking about the influence of non-carbohydrate nutrients and (b) "[n]o clear association between SFA intake relative to refined carbohydrates and the risk of insulin resistance
and diabetes has been shown" (Astrup. 2011), we will probably have to resort to protein (see last installment) or mono- and polyunsaturated fatty acids. Both have been shown to exert beneficial effects on glucose and lipid homeostasis, as well as other important health markers.- MUFAs boost resting energy expenditure: Next to its beneficial effects on blood glucose and lipid management, a high intake of monounsaturated fatty acids can also increase the resting energy expenditure in humans by 3% in the fed and 4% in the fasted state, respectively (Kien. 2013).Monounsaturated fats - MUFAs -- Gadgil et al. report that 2 weeks on high MUFA diets lead to prompt improvements in insulin sensitivity in 64 individuals with prehypertension or stage 1 hypertension without diabetes (Gadgil. 2013). Two years before Gillinghan et al. wrote in a review of the effect of high mono-unsatuarated fatty acid intakes that the "[c]onsumption of dietary MUFA promotes healthy blood lipid profiles, mediates blood pressure, improves insulin sensitivity and regulates glucose levels" (Gillingham. 2011).
- Polyunsaturated fats = PUFAs -- Similar beneficial effect on heart health have been reported for the replacement of saturated fat with polyunsaturated fatty acids (both, omega-3 and omega-6; see Flock. 2014). Evidence for the beneficial effects of omega-3 fatty acids, in particular, dates back to the late 1980s, when Popp-Snijders et al. observed that 8 weeks of daily supplementation of 3 g of the omega 3 fatty acids eicosapentaenoic and docosahexaenoic acid improves the insulin sensitivity of subjects with non-insulin-dependent diabetes (Popp-Snijders. 1987).
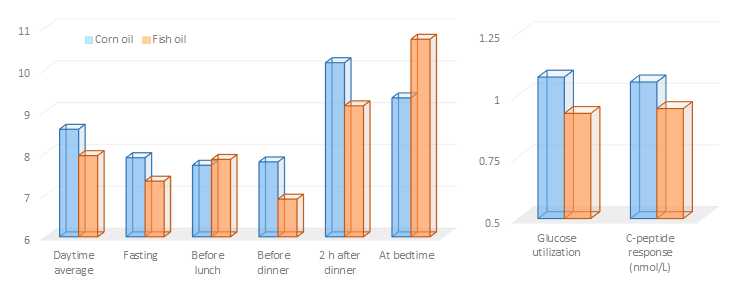
Unfortunately, studies like this have triggered an unwarranted euphoria even among healthy individuals, whose hope for further improvements in insulin sensitivity are not just unwarranted (Risérus. 2008), but could actually mislead them to mimic the high-dose fish oil supplementation regimen of the diabetic subjects in a 2006 study by Mostad et al. (1.8 g 20:5n−3, 3.0 g 22:6n−3, and 5.9 g total n−3 fatty acids from fish oil) to end up with a similar negative effect on blood glucose levels and glucose utilization (see Figure 1).
It must be said, though, that the Mostad study is an exception. Most fish oil supplementation studies used lower amounts of fish oil and showed improvements in lipid metabolism, but no effect on insulin sensitivity, similar to those Kabir et al. observed in 2007. Accordingly, reviewers agree fish oil supplementation in moderate dosages (equivalent to 1-2 g/day n-3 LCPUFA) has no significant adverse effects on fasting glucose, HbA1c, fasting insulin, or insulin sensitivity (McManus. 1996; Friedberg. 1998; Montori. 2000; Lombardo. 2006; Akinkuolie. 2011; Lee. 2013) - unfortunately, it does not improve these parameters, either.
Figure 1: Blood glucose levels (left), glucose utilization and C-peptide levels (right) of 26 diabetic subjects after 8 weeks of high dose fish oil vs. corn oil supplementation (Mostad. 2006)
Are transfats fat burners? It is certainly counter-intuitive, but in the Lovejoy study, the 9% transfat (elaidic acid) diet did not leave the insulin sensitivity of the 25 healthy men and women who participated in the trial unchanged, they did also increase the oxidation of fatty acids by 21% compared to the high MUFA diet (Lovejoy. 2002).
If we compare the results of the Lovejoy study to those Vesby et al. present in their 2001 paper, it would appear that the perviously cited 10% of the total energy intake could actually be a realistic upper intake level. With 17% of the total energy the diet in Vesby's 3 months study had a significantly higher saturated fat content - high enough to produce a -10% reduction in insulin sensitivity compared to baseline (-12% compared to high MUFA control). Similar negative effects have been observed in the Rosquist (2014) study, I wrote about only a couple of days ago (see "Saturated Fat Makes You Fat!" | read more).This wouldn't be the SuppVersity, though, if I didn't list at least two of the "on the other hands" we haven't discussed yet. Firstly, there are no long-term dietary intervention studies that would support the results of these and other 4-12 week interventions.
Is palmitic acid the bad guy? If SFAs impair insulin action, are all SFAs equally bad? Possibly not, but there is still insufficient evidence to prove this. Vessby et al. proposed that especially high proportions of palmitic acid may promote insulin resistance, and that a major role of SCD-1 may be to reduce the availability of palmitic acid in body tissues by converting it to palmitoleic acid. And while it appears as if palmitic acid had most significant negative effects on cellular glucose transport, fat oxidation, ceramide synthesis, cellular signalling, apoptosis and lipogenesis, conclusive evidence that "it's just palmitic acid that's the problem", is still missing.
And secondly, and probably more importantly, none of the studies investigated the interactions between the saturated fat and carbohydrate content of the diets. As I pointed out right at the beginning of this article, there is little doubt that a high fat diet with a minimal carbohydrate content will lower the average blood glucose levels of (pre-)diabetic individuals - in this case, the negative effects of palmitic acid on the insulin sensitivity of skeletal muscle (Sawada. 2012), fat cells (Kennedy. 2009), and the hypothalamus (Benoit. 2011) are irrelevant, anyway. No carbs, no increase in blood glucose, no need for insulin stimulated glucose uptake... ah, and not a topic for this article series, since it is about the influence of "non-carbohydrate" nutrients on blood glucose levels.Another of these non-carbohydrate nutrients that got an honorable mention as purported fat burner in a couple of paragraphs before are cis- and transfats. Isomeric fatty acids with the same number of carbon and hydrogen atoms, but very distinct health effects. Transfats include:
- "unnatural" cis- and trans monounsaturated fatty acids as they occur in partially hydrogenated fats, but also
- "natural" ones such as vaccenic acid and the conjugated isomers of linoleic acid (CLA) in dairy
Before we are taking a closer look at how bad the "bad" unnatural transfats actually are, I would thus like to suggest that we remind ourselves of the benefits of their ruminant cousins.
 |
| Contrary to the benefits of supplemental CLA, the beneficial effects of vaccenic acid and other ruminant transfats in dairy are beyond doubt | more |
Only a couple of days ago, on Friday, to be precise, I posted a blurb about a recent study from the Konkuk University in Korea, which demonstrated direct anti-cancer effects from the "CLA precursor" vaccenic acid (Lim. 2014). The #1 ruminant transfat in full-fat milk and dairy products (read more on the SuppVersity Facebook Page).
 |
| If you wanted to destroy your body fat, you'd have to consume exclusively the prodiabetic, inflammatory tans-10, cis-12 isomer | learn more |
Surprise: No evidence to support benefit of reduction of dietary TFA on glucose homeostasis
If we take a look at the corresponding effects of transfats, the picture that emerges is less clear. A recent meta-analysis ofseven randomized, placebo-controlled clinical trials, for example, has shown that an increase in TFA intake from 2.6% to 7.8% of total energy intake did not lead to any significant change in circulating glucose or insulin concentrations (Aronis. 2012). The meta-regression analysis the researchers from the Harvard Medical School conducted also revealed that there was no dose-response relationship between the amount of transfats their subjects consumed and the corresponding effects on blood glucose and insulin concentrations. In spite of the very real detoriations of the HDL/LDL cholesterol ratio, there is thus, as Aronis et al. rightly point out, "no evidence to support a potential benefit of the reduction of dietary TFA intake on glucose homeostasis." (Aronis. 2012)
Let's not forget the acute effects!
I mentioned them right at the beginning of this article: The acute effects dietary fats can and will have on the blood glucose, insulin and incretin (~satiety hormone) response to a meal.
 |
| Figure 2: Blood glucose (mmol/L, left), GIP (pmol/L, top-right), and insulin (mU/L, bottom-right) response to a standardized mashed potato meal 30min after the ingestion of water, olive oil, or both (Gentilcore. 2006) |
The pro-inflammatory effects of high fat meals, of which a recent paper by Mohammed Herieka and Clett Erridge would suggest that they have been underestimated in the common analyses of plasma borne markers of inflammation, such as cytokines and soluble adhesion molecules (Herieka. 2014), on the other hand depend largely on the type of dietary fat that is consumed. While cooking oils and foods that are high in saturated fats appear to have consistent pro-inflammatory effects (Williams. 1999), high MUFA and or omega-3 enriched meals, walnuts, almonds, pistachios and, obviously, fatty fish will ameliorate the postprandial inflammation and exert beneficial effects on the vascular reactivity (West. 2005).
 |
| Figure 3: Pro-inflammatory dietary fats are only one of the components that drive the contribution of the postprandial inflammatory response to the self-intensifying circle of metabolic inflammation (Margioris. 2009) |
Don't worry if your head feels ready to explode
It's about time, we sum things up, anyway. While we certainly have a lot to learn, the contemporary scientific evidence would suggest that...
- the commonly cited negative effects of dietary fat on insulin sensitivity are real - even a high fat, low carb diets will lead to acute reductions in glucose tolerance (Hales. 1963),
- the negative effects on insulin sensitivity are partially mediated by increases in free fatty acids (Roden. 1996),
- the ill health effects of the high fat-induced reduction in glucose tolerance depends on the presence and amount of carbohydrates, as well as the total energy intake and -expenditure and other non-nutrient dependent parameters (Margois. 2009),
- in the postprandial phase, the impaired / slowed influx of glucose and the prolongation of the postprandial hyperinsulinemia may provide an acute relief for people with already elevated blood glucose levels (Gentilcore. 2006), eventually, they will yet promote the development and progression of insulin resistance (Marangou. 1986)
the postprandial inflammation that occurs after the ingestion of a high fat meal is problematic for individuals with an already high baseline inflammation (Peairs. 2011),
Figure 4: Insulin secretion rates in response to isocaloric meals based water (CONT), palm oil (SFA), olive oil (MUFA) and safflower oil (PUFA) in overweight and obese but otherwise health non-diabetic men (Xiao. 2006) - based on epidemiological evidence it would appear that the replacement of saturated with mono-unsaturated fats will result in long-term improvements in blood glucose management (Gillingham. 2011),
- compared to saturated fat, an increase in polyunsaturated fats improves the acute insulin response to an otherwise isocaloric meal (see Figure 4; safflower vs. olive vs. palm oil in Xiao. 2006),
- the anti-inflammatory effect of omega-3 fatty acids do not produce consistent improvements in blood glucose management (Akinkuolie. 2011),
there are concerns that very high intakes of omega-3 fatty acids (>6g of LCPUFA for months) could lead to reductions in insulin sensitivity similar to those we are seeing with the imbalanced omega-6 intake of the Western diet (Simopoulos. 2002; Mostad. 2006),
Figure 5: Paleo-lovers listen up! Aside from a higher protein and a sign. lower N6/N3 ratio, the alleged "paleo diet" or rather the diet, Cordain, Eaton & co tell you our ancestors ate had a 50% lower SFA:PUFA ratio (Simopoulos. 2002) - the anti-diabetes effects of high(er) PUFA intakes come hand in hand with a pro-obesogenic increase in PPAR-gamma activity similar to, but less pronounced than those of thiazolidinedione-based anti-diabetes drugs like pioglitazone - keyword: "obese, but healthy"
- the existence and even more so the extent of the often-claimed negative effects of transfats on glucose metabolism are dubious (Aronis. 2012); if anything, they occur as long(er) term down-stream effects of more general pro-inflammatory and hyperlipidemic effects of non-ruminate trans fatty acids and the foods that contain them (Remig. 2010), and lastly
- there is accumulating evidence that the natural blend of ruminant transfats in high fat dairy exerts beneficial effects on glucose metabolims (Mensink. 2005; Lim. 2014)


 |
| The superior lean mass and significantly reduced fat gains, Mendes-Netto et al. observed in 2011 with an extreme high carb + low fat diet are a perfect example of the fact you better stay away from fat, when you feel the need to overeat on carbs on a bulk or whenever else | more. |
In concert with a balanced whole-foods diet, regular physical activity and quality sleep, however, your health and insulin sensitivity are not going to be threatened by the consumption of reasonable amounts of saturated fats and their potentially pro-inflammatory omega-6 cousins whose overabundance and not their inclusion in the modern Western is a highly obesogenic problem (see Figure 5).
- Akinkuolie, Akintunde O., et al. "Omega-3 polyunsaturated fatty acid and insulin sensitivity: a meta-analysis of randomized controlled trials." Clinical Nutrition 30.6 (2011): 702-707.
- Aranceta, Javier, and Carmen Pérez-Rodrigo. "Recommended dietary reference intakes, nutritional goals and dietary guidelines for fat and fatty acids: a systematic review." British Journal of Nutrition 107.S2 (2012): S8-S22.
- Astrup, Arne, et al. "The role of reducing intakes of saturated fat in the prevention of cardiovascular disease: where does the evidence stand in 2010?." The American journal of clinical nutrition 93.4 (2011): 684-688.
- Benoit, Stephen C., et al. "Palmitic acid mediates hypothalamic insulin resistance by altering PKC-θ subcellular localization in rodents." The Journal of clinical investigation 121.1 (2011): 456.
- Carlson, Susan E., Jane D. Carver, and Stephen G. House. "High fat diets varying in ratios of polyunsaturated to saturated fatty acid and linoleic to linolenic acid: a comparison of rat neural and red cell membrane phospholipids." The Journal of nutrition 116.5 (1986): 718-725.
- den Besten, Gijs, et al. "The role of short-chain fatty acids in the interplay between diet, gut microbiota, and host energy metabolism." Journal of lipid research 54.9 (2013): 2325-2340.
- Flock, Michael R., Jennifer A. Fleming, and Penny M. Kris-Etherton. "Macronutrient replacement options for saturated fat: effects on cardiovascular health." Current opinion in lipidology 25.1 (2014): 67-74.
- Friedberg, Cylla E., et al. "Fish oil and glycemic control in diabetes: a meta-analysis." Diabetes Care 21.4 (1998): 494-500.
- Gadgil, Meghana D., et al. "The Effects of Carbohydrate, Unsaturated Fat, and Protein Intake on Measures of Insulin Sensitivity Results from the OmniHeart Trial." Diabetes care 36.5 (2013): 1132-1137.
- Gentilcore, Diana, et al. "Effects of fat on gastric emptying of and the glycemic, insulin, and incretin responses to a carbohydrate meal in type 2 diabetes." Journal of Clinical Endocrinology & Metabolism 91.6 (2006): 2062-2067.
- Gillingham, Leah G., Sydney Harris-Janz, and Peter JH Jones. "Dietary monounsaturated fatty acids are protective against metabolic syndrome and cardiovascular disease risk factors." Lipids 46.3 (2011): 209-228.
- Grygiel-Górniak, Bogna. "Peroxisome proliferator-activated receptors and their ligands: nutritional and clinical implications-a review." Nutrition journal 13.1 (2014): 17.
- Halade, Ganesh V., Md M. Rahman, and Gabriel Fernandes. "Differential effects of conjugated linoleic acid isomers in insulin-resistant female C57Bl/6J mice." The Journal of nutritional biochemistry 21.4 (2010): 332-337.
- Hales, C. N., and P. J. Randle. "Effects of low-carbohydrate diet and diabetes mellitus on plasma concentrations of glucose, non-esterified fatty acid, and insulin during oral glucose-tolerance tests." The Lancet 281.7285 (1963): 790-794.
- Harvey, Kevin A., et al. "Long-chain saturated fatty acids induce pro-inflammatory responses and impact endothelial cell growth." Clinical Nutrition 29.4 (2010): 492-500.
- Herieka, Mohammed, and Clett Erridge. "High‐fat meal induced postprandial inflammation." Molecular nutrition & food research 58.1 (2014): 136-146.
- Kennedy, Arion, et al. "Saturated fatty acid-mediated inflammation and insulin resistance in adipose tissue: mechanisms of action and implications." The Journal of nutrition 139.1 (2009): 1-4.
- Khan, Mehmood A., John V. St Peter, and Jay L. Xue. "A prospective, randomized comparison of the metabolic effects of pioglitazone or rosiglitazone in patients with type 2 diabetes who were previously treated with troglitazone." Diabetes Care 25.4 (2002): 708-711.
- Kien, C. Lawrence, et al. "Substituting dietary monounsaturated fat for saturated fat is associated with increased daily physical activity and resting energy expenditure and with changes in mood." The American journal of clinical nutrition 97.4 (2013): 689-697.
- Kimura, Ikuo, et al. "The gut microbiota suppresses insulin-mediated fat accumulation via the short-chain fatty acid receptor GPR43." Nature communications 4 (2013): 1829.
- Kota, Bhavani Prasad, Tom Hsun-Wei Huang, and Basil D. Roufogalis. "An overview on biological mechanisms of PPARs." Pharmacological Research 51.2 (2005): 85-94.
- Lombardo, Yolanda B., and Adriana G. Chicco. "Effects of dietary polyunsaturated n-3 fatty acids on dyslipidemia and insulin resistance in rodents and humans. A review." The Journal of nutritional biochemistry 17.1 (2006): 1-13.
- Lemaitre, Rozenn N., et al. "Cell membrane trans-fatty acids and the risk of primary cardiac arrest." Circulation 105.6 (2002): 697-701.
- Lovejoy, Jennifer C., et al. "Effects of diets enriched in saturated (palmitic), monounsaturated (oleic), or trans (elaidic) fatty acids on insulin sensitivity and substrate oxidation in healthy adults." Diabetes care 25.8 (2002): 1283-1288.
- Marangou, A. G., et al. "Metabolic consequences of prolonged hyperinsulinemia in humans: evidence for induction of insulin insensitivity." Diabetes 35.12 (1986): 1383-1389.
- Margioris, Andrew N. "Fatty acids and postprandial inflammation." Current Opinion in Clinical Nutrition & Metabolic Care 12.2 (2009): 129-137.
- McManus, Ruth M., et al. "A comparison of the effects of n-3 fatty acids from linseed oil and fish oil in well-controlled type II diabetes." Diabetes Care 19.5 (1996): 463-467.
- Mendes-Netto, R. S., et al. "Effect of the dietary glycid/lipid calorie ratio on the nitrogen balance and body composition of bodybuilders." Nutrire-Revista da Sociedade Brasileira de Alimentação e Nutrição 36.1 (2011): 137-150.
- Mensink, Ronald P. "Metabolic and health effects of isomeric fatty acids." Current opinion in lipidology 16.1 (2005): 27-30.
- Kabir, Morvarid, et al. "Treatment for 2 mo with n− 3 polyunsaturated fatty acids reduces adiposity and some atherogenic factors but does not improve insulin sensitivity in women with type 2 diabetes: a randomized controlled study." The American journal of clinical nutrition 86.6 (2007): 1670-1679.
- Lee, C., et al. "Fish consumption, insulin sensitivity and beta-cell function in the Insulin Resistance Atherosclerosis Study (IRAS)." Nutrition, Metabolism and Cardiovascular Diseases 23.9 (2013): 829-835.
- Lim, Ji-Na, et al. "trans-11 18: 1 Vaccenic Acid (TVA) Has a Direct Anti-Carcinogenic Effect on MCF-7 Human Mammary Adenocarcinoma Cells." Nutrients 6.2 (2014): 627-636.
- Mahendran, Yuvaraj, et al. "Association of erythrocyte membrane fatty acids with changes in glycemia and risk of type 2 diabetes." The American journal of clinical nutrition 99.1 (2014): 79-85.
- Montori, Victor M., et al. "Fish oil supplementation in type 2 diabetes: a quantitative systematic review." Diabetes Care 23.9 (2000): 1407-1415.
- Mostad, Ingrid L., et al. "Effects of n− 3 fatty acids in subjects with type 2 diabetes: reduction of insulin sensitivity and time-dependent alteration from carbohydrate to fat oxidation." The American journal of clinical nutrition 84.3 (2006): 540-550.
- Peairs, Abigail D., Janet W. Rankin, and Yong Woo Lee. "Effects of acute ingestion of different fats on oxidative stress and inflammation in overweight and obese adults." Nutr J 10.1 (2011): 122.
- Poirier, Hélène, et al. "Nutritional supplementation with trans-10, cis-12–conjugated linoleic acid induces inflammation of white adipose tissue." Diabetes 55.6 (2006): 1634-1641.
- Popp-Snijders, C., et al. "Dietary supplementation of omega-3 polyunsaturated fatty acids improves insulin sensitivity in non-insulin-dependent diabetes." Diabetes Research (Edinburgh, Scotland) 4.3 (1987): 141-147.
- Remig, Valentina, et al. "Trans Fats in America: A Review of Their Use, Consumption, Health Implications, and Regulation." Journal of the American Dietetic Association 110.4 (2010): 585-592.
- Risérus, Ulf, et al. "Treatment with dietary trans10cis12 conjugated linoleic acid causes isomer-specific insulin resistance in obese men with the metabolic syndrome." Diabetes care 25.9 (2002): 1516-1521.
- Risérus, Ulf. "Fatty acids and insulin sensitivity." Current Opinion in Clinical Nutrition & Metabolic Care 11.2 (2008): 100-105.
- Roden, Michael, et al. "Mechanism of free fatty acid-induced insulin resistance in humans." Journal of Clinical Investigation 97.12 (1996): 2859.
- Sawada, Keisuke, et al. "Ameliorative effects of polyunsaturated fatty acids against palmitic acid-induced insulin resistance in L6 skeletal muscle cells." Lipids Health Dis 11.1 (2012): 36-44.
- Simopoulos, Artemis P. "The importance of the ratio of omega-6/omega-3 essential fatty acids." Biomedicine & pharmacotherapy 56.8 (2002): 365-379.
- Schwingshackl, L., B. Strasser, and G. Hoffmann. "Effects of monounsaturated fatty acids on glycaemic control in patients with abnormal glucose metabolism: a systematic review and meta-analysis." Annals of Nutrition and Metabolism 58.4 (2011): 290-296.
- Vessby, Bengt, et al. "Substituting dietary saturated for monounsaturated fat impairs insulin sensitivity in healthy men and women: The KANWU Study." Diabetologia 44.3 (2001): 312-319.
- Williams, Michael JA, et al. "Impaired endothelial function following a meal rich in used cooking fat." Journal of the American College of Cardiology 33.4 (1999): 1050-1055.
- Xiao, C., et al. "Differential effects of monounsaturated, polyunsaturated and saturated fat ingestion on glucose-stimulated insulin secretion, sensitivity and clearance in overweight and obese, non-diabetic humans." Diabetologia 49.6 (2006): 1371-1379.


